As we age it is normal for our retina to lose some of its sensitivity over time. Some of us experience an above normal rate of decline in our central vision, called Macular Degeneration ( also known as ARMD - Age Related Macula Degeneration, previously known as SMD - senile macular degeneration or AMD). ARMD is devided into two main types, dry macular degeneration and wet macular degeneration.
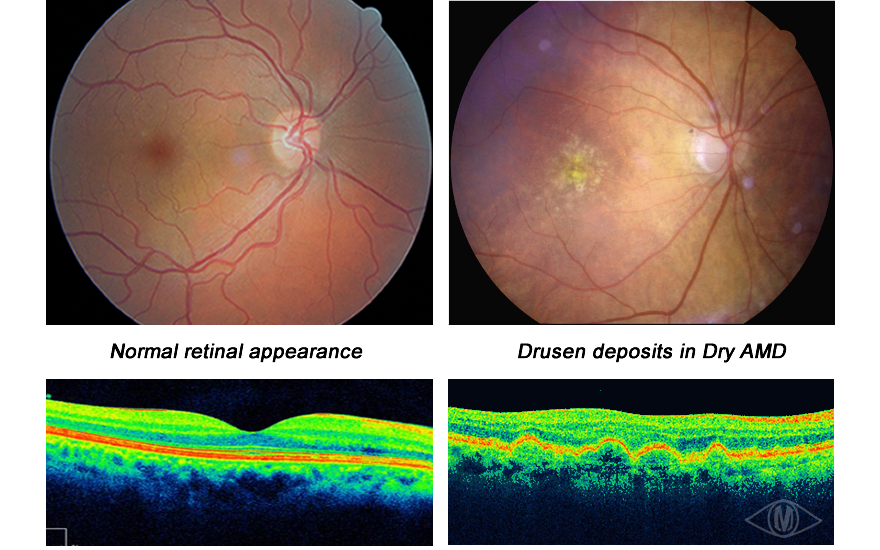
Dry macula degeneration has 2 main subtypes, Drusen based and Atrophy based. In Drusenoid macula degeneration there is a gradual accumulation of the various waste products from the process of seeing in the retina at the level of the Retinal Pigment Epithelium which lies just underneath the photo-receptors. the presence of these drusen deposits can disrupt the normal regular spacing of the photo-receptors and distort our central vision. This process is normally slow and currently the only proven way to attempt to slow down the progression of this build up is to take an antoxident vitamin/mineral supplement such as Visionace (this is available from our on-line shop).
The other form of age related macular degeneration is called Atrophic Macular Degeneration. In this type the photoreceptors and their pigments waste or atrophy away, thereby reducing macular sensitivity. There is research at present to see if taking oral supplements of these pigments helps reduce the speed at which they leach out of the retinal tissues.
Certain of these waste products that build up in the retina can now be picked up much earlier than previously by a technique called Autofluorescence Photography. Matheson Optometrists are working with retinal camera developers to develop a camera system for this purpose. When Lipofusin in the retina is illuminated with a particular wavelength of visible light, usually a greenish-blue colour, it fluoresces, or glows with a different wavelenth of light. By the clever use of exciter and barrier filters, it is possible to photograph this emmitted light of different colour, which gives us a measure of how much lipofusin is present in the retina.
Currently, the most efficient way we can detect and monitor Macula changes is the use of our Ocular Coherence Tomography equipment. Please click here for more information.
New exciting research and clinical studies have found red light to also be of benefit in Dry Macular Degeneration. Improvements in vision and retinal anatomy have been achieved by decreasing the inflammation and recovering blood flow. Initial studies show a rapid effect, decreasing drusen, increasing blood flow and improved visual acuity which is maintained for over six months
tttttttttttttt
Photobiomodulation (PBM) is a light-based therapy showing significant promise in the potential treatment of dry AMD. Therapy is delivered via the LumiThera Valeda device. Andrew Luff and Deb Sahu are specialist retinal consultants at Sapphire Eyecare treatment unit, based at Highcliffe Medical Centre, where this new treatment is now available.
Dry AMD has remained frustratingly resistant to intervention in spite of our massively increased knowledge of retinal pathophysiology, genetics and inflammatory pathways.
Light therapy, primarily with red and near-infrared wavelengths, has been shown beneficial for a number of pathologies throughout the body. The science of photobiomodulation (PBM) is developing rapidly with recent publications demonstrating impressive short-term results in the earlier stages of dry AMD. A 2017 paper (Merry GF et al. Acta Ophthalmologica. 2017: 95: e270-277), showed improvement in both retinal morphology and visual function (particularly contrast sensitivity) following a short course of treatment. Photobiomodulation reduces drusen volume and improves visual acuity and contrast sensitivity in dry age-related macular degeneration.
Initial studies show a rapid effect with benefit maintained over six months. A second treatment at that point appeared once again to deliver a positive result but no longer-term data are, as yet, available. Further clinical trials are in progress but, given the weight of evidence and the current lack of any other effective treatment, this minimally invasive and very low-risk treatment appears worthy of consideration.
Scientific background:
Experimental work and clinical studies have demonstrated the potential for red light to benefit retinal function in AMD, leading to both anatomical improvement and visual gain. The treatment is thought to work through improvement in blood flow, decreased inflammation and increased mitochondrial function. Recent studies of patients with AMD have concentrated on dry disease, but earlier studies also show certain benefits for patients with wet AMD.
Patient selection
Suitable patients should have evidence of AMD sufficient to be considered for AREDS supplements. Visual acuity should be 6/36 or better in at least one eye. Patients judged to have significant cataract may undergo surgery after the initial treatment cycle. Those with bilateral AMD developing wet change in one eye may have bilateral treatment, but patients with bilateral wet AMD will be excluded until further data are available. Anti-VEGF injection should continue as directed by the treating centre.
Treatment protocol
A therapy cycle consists of three treatments per week for three consecutive weeks. Measurement visual acuity along with retinal photography and OCT scanning will be performed six weeks after the start of treatment.
On-going treatments
Further treatment cycles may be required after an interval of six months