Auto-Fluorescence in Clinical Practice using a modified Canon Retinal Camera
By Andrew Matheson extract from article published in Optician magazine
Fundus Auto-Fluorescence (FAF) imaging is probably the most exciting new affordable clinical technology to arrive in optometric practice since the OCT.
Lipofusin is a pigment which glows, or Auto-fluoresces, with a reddish golden yellow colour if excited with a blue green light. We can thus evaluate the amount of Lipofuscin present in the retina. This is the basis of FAF imaging. Lipofuscin exhibits a broad emission spectrum from 500 to 750 nm with peak emission at about 630 nm.(ref 1)
The RPE digests the by-products of the visual cycle generally very efficiently by phagocytosis. There is a small proportion of the degradation products from the phagocytosed outer segments of the rods and cones and mitochondria that cannot be eliminated. This accumulates in the lysosymes of the RPE as Lipofuscin and related products.
Lipofuscin deposition normally increases with age, but may also occur from RPE cell dysfunction or an abnormal metabolic load on the RPE. The dominant fluorophore in lipofuscin is believed to be A2-E, a compound that may interfere with normal RPE cell and photoreceptor function, by producing toxic oxidative radicals, when stimulated by light. (ref 2,3). After the age of 70 lipofuscin levels level out or sometimes even decline. We are not sure exactly why this occurs, but may be due to evacuation of the lipofuscin into the extravascular space as precursor material leading to drusen formation.
As an independent prescriber I work closely with local vitreo-retina and medical-retina specialists. One of our main concerns was to try to identify which of our early dry macular degeneration patients were at high risk of visual loss and needed aggressive management. Auto-Fluorescence gives us an additional tool to categorise our dry ARMD patients into high and low risk groups, after taking into account all the other risk factors.
The optic disc and blood vessels appear dark in an autofluorescence picture, more so with the cSLO than the retinal camera version. The optic disc has no lipofuscin and the retinal vessels mask the autofluorescence from the deeper layers.
The FAF is less intense in the foveal region probably due to the protective effect of the macular pigments, lutein, zeaxanthin and the RPE melanin. Another possible explanation is that the cone phagocytosis may produce less lipofuscin than that of the rods.
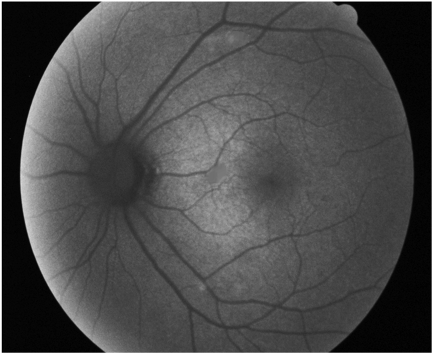
In the normal retina of a 40-year old the AF retinal photo has a uniform grey background colour (fig 1).
fig 1 Normal Retinal Auto-Fluorescence Appearance
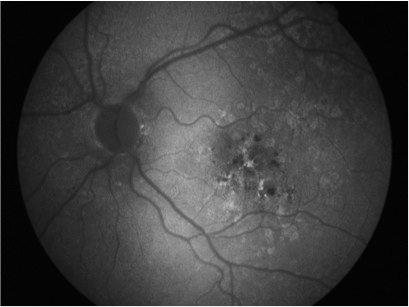
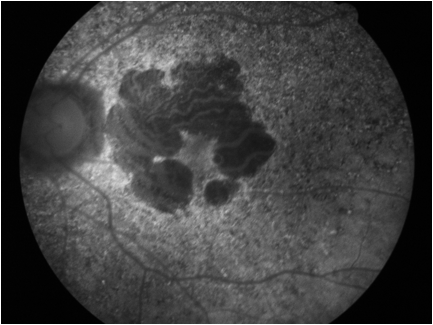
In a “sick” retina the Lipofuscin first builds up into clumps of Hyper-Autofluorescence, which shows as brighter white patches against the uniform grey background (see fig 2). As the RPE cells deteriorate further, the hyper-fluorescent white areas often become Hypo-fluorescent dark patches as the RPE atrophies. As the atrophy progresses the dark, lipofuscin-free patches grow in size, reflecting the true visual state of the retina, not always obvious when viewed by other means (see fig 3).
Fig 2 showing Retinal Auto-Fluorescence Appearance in ARMD with both hyper-fluorescent and hypo-fluorescent lesions
In early ARMD focally increased AF appears to indicate the likely progression to Geographic Atrophy, rather than CNV as the mechanism of further visual loss.
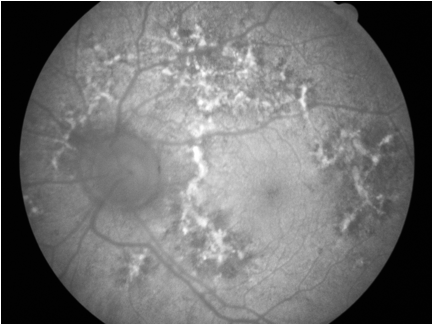
A reduction in AF indicates loss of either RPE or photoreceptor/photoreceptor outer segments. This loss often appears subtle on biomicroscopy or standard retinal photography and can be easily missed(see colour photo fig xxx below). AF photography shows such defects up clearly, giving us a better understanding of outer retinal health. In fig 4 which clearly shows areas of extensive atrophy surrounded by “hot-spots” of lipofuscin accumulation, indicating areas likely to atrophy in near future(ref 7).
fig 3 Apparantly “normal” retinal appearance at first glance
fig 4 Same eye as fig 3, FAF demonstrates significant geographic atrophy
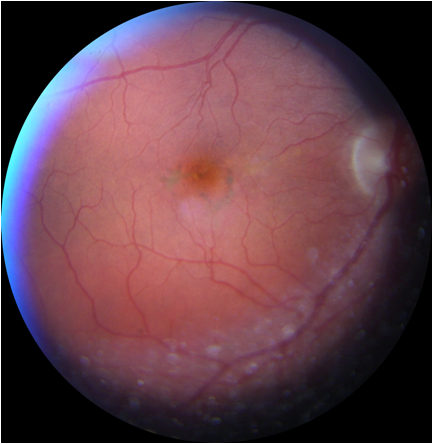
In the next two photos, first see an apparently “normal” colour fundus appearance(fig 4) in contrast to the definitely “abnormal” FAF photo taken of the same eye minutes afterwards(fig 5). This shows the time bomb effect the accumulating lipofuscin has on the retinal pigment epithelium, which before we had FAF imaging we were blissfully unaware of.
fig 5 Apparently “normal retinal appearance
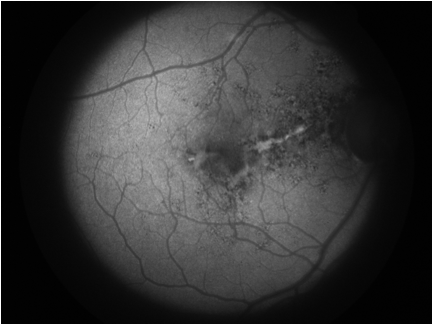
fig 6 FAF shows otherwise
In this next colour photo we see early macular pigment mottling, but little else to indicate the changes at RPE level shown by the following FAF image.
fig 7, early pigment mottling
fig 8, FAF shows fuller picture
It is the accumulation of lipofuscin in Stargart’s Macular Degeneration that is thought to be implicated in the characteristic atrophy seen in this condition (see figs 9-16). The bright flecks often seen in Stargardts Diseaseare shown histologically to be RPE cells so engorged with Lipofuscin that they become distorted to 10x their normal size(ref 9).
It is is likely that the damage is caused by the release of oxidative radicals on photo-stimulation of the lipofuscin pigment. The highest levels of oxidative radicals being produced at high light intensities and shorter blue end of the visual spectrum. There is evidence that the photo-activity of lipofuscin increases with age, thereby increasing the oxidative damage it can cause.