For some people, surgery might be the best treatment for glaucoma. Your ophthalmologist may suggest surgery as a first treatment, or after trying medication to lower your IOP.
There are several different types of surgery for glaucoma. The kind of surgery you and your ophthalmologist decide is right for you depends on many factors, including the type and severity of your glaucoma, and other eye problems or health conditions.
Glaucoma surgery may be performed using a laser (a concentrated beam of light) or conventional surgical instruments.
Trabeculoplasty is used most often to treat open-angle glaucoma. In trabeculoplasty, a laser is used to place "spot welds" in the drainage area of the eye-- also known as the trabecular meshwork -- that allow the aqueous to drain more freely.
Iridotomy is another kind of laser surgery used in treating glaucoma. It is frequently used to treat angle-closure glaucoma. In this procedure, the surgeon uses the laser to make a small hole in the iris-- the colored part of the eye -- which allows the aqueous to flow more freely within the eye so the iris doesn't plug up the trabecular meshwork.
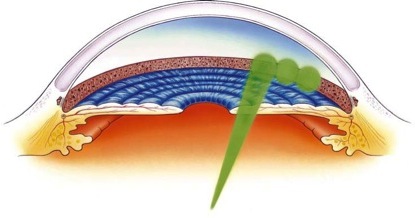
In cyclophotocoagulation, a laser beam is used to freeze selected areas of the ciliary body -- the part of the eye that produces aqueous humor -- to reduce the production of fluid. This procedure may be used to treat more advanced or aggressive cases of glaucoma.
Most laser surgeries for glaucoma can be performed in the ophthalmologist's office or an outpatient surgical facility. Eye drops are used to numb the eye for the duration of the procedure. Because there is usually little discomfort during glaucoma surgery, this is often the only anesthesia needed
Little recuperation is needed after laser eye surgery. Patients may experience some local eye irritation, but can usually resume their normal activities a day or two after surgery.
In some cases, laser surgery is not the preferred surgical treatment for glaucoma. Sometimes, when vision loss is rapid, or medication and/or laser surgery fails to lower IOP sufficiently, "conventional" incisional surgery is the best option.
Incisional Surgery
If eye drops or laser therapy have not succeeded in lowering the eye pressure, the doctor may recommend an operation to control the pressure. The most common operation is called trabeculectomy.
The eye has a tough outer wall (the sclera) which is covered by a thinner skin (the conjunctiva). In a trabeculectomy, the surgeon makes a flap over a small hole in the sclera. The flap forms a new passage for aqueous humour to leave the eye under the conjunctiva.
The trabeculectomy forms a small bump under the upper lid, called a trabeculectomy bleb. Sometimes is may be possible to see fine stitches. These stitches hold the flap in place.
The operation may be performed under local anaesthesia or general anaesthetic. With local anaesthetic, an injection is given next to the eye to numb the eye and you are awake during the operation (but you do not see what is going on). With general anaesthesia, you are asleep during the operation.
How successful is the operation likely to be?
Five years after surgery, the eye pressure remains controlled in about 75 per cent of patients. If the operation fails to control the pressure some time after the surgery, the operation may be repeated or drops can be started again.
Some patients produce more scar tissue than other patients and the scar tissue may block the flap and prevent the operation working. If scarring is likely, the surgeon may recommend the use of anti-scarring treatment at the time of, or shortly after, the surgery.
Side effects and complications
Trabeculectomy may cause an existing cataract to develop more quickly. A cataract occurs when the lens in your eye becomes cloudy. This causes the vision to become misty and less clear. Cataract surgery – the replacement of your natural lens with a clear artificial lens – can be performed after a trabeculectomy.
There is a long-term risk of getting an infection in the eye after trabeculectomy. If you develop a red, sore eye at any time after the operation, then you should see an eye doctor immediately.
In some patients, a trabeculectomy is not the best operation and other forms of surgery maybe performed. These include viscocanalostomy, deep sclerectomy and 'tube' or 'valve' operations.
Viscocanalostomy
Viscocanalostomy is a relatively new technique developed for glaucoma surgery and was first proposed in 1991.
Whereas a trabeculectomy creates a 'flap' in the eye, allowing the aqueous humour to drain directly from the front of the eye to form a bleb under the conjunctiva, viscocanalostomy does not involve making a full-thickness hole into the front of the eye. Instead, the surgeon removes a block of sclera to leave a thin membrane (Descemet's membrane) through which the aqueous humour percolates. The aqueous then drains away either through Schlemm's canal (in the natural way) or under the conjunctiva. During the surgery, a thick fluid (visco-elastic) is injected into Schlemm's canal, hence the name of the operation – viscocanalostomy.
There are theoretical advantages over a trabeculectomy, such as a reduced rate of cataract development and lower risk of excessively low pressure after surgery. However, the amount by which the eye pressure is lowered by viscocanalostomy is not usually as great as that by trabeculectomy.
Deep Sclerectomy
The deep sclerectomy operation is essentially very similar to the viscocanalostomy operation, with similar advantages and disadvantages.
It is usually performed with the insertion of a material (collagen implant) under the scleral flap to improve the drainage of aqueous humour under the conjunctiva.
'Tube' or 'Valve' operations
In these procedures, the surgeon places a small plastic tube in the eye. This allows fluid to drain out of the eye to a special reservoir under the conjunctiva (skin of the eye). This is usually hidden under the top eye lid. The fluid is absorbed from the reservoir back into the bloodstream.
Filtering surgery is usually done in a hospital or outpatient surgery center, with local anesthesia, and sometimes, sedation. The surgeon uses very delicate instruments to remove a tiny piece of the wall of the eye (the sclera), leaving a tiny hole. The aqueous can then drain through the hole, reducing the intraocular pressure, and be reabsorbed into the bloodstream.
In some cases, the surgeon may place a small tube or valve in the eye through a tiny incision in the sclera. The valve acts a regulator for the buildup of aqueous within the eye. When the intraocular pressure reaches a certain level, the valve opens, allowing the fluid to flow out of the eye's interior, where it can be reabsorbed by the body. The procedure may take place in the ophthalmologist's office or outpatient surgical center, and can be done under local anesthesia.
The recuperative period following incisional glaucoma surgery is usually short. You may need to wear an eye patch for a few days after surgery, and to avoid activities which expose the eye to water, such as showering or swimming. The ophthalmologist may recommend you refrain from heavy exercise, straining or driving for a short time after surgery, to avoid complications.
Possible Complications
As with all surgery, there are risks associated with glaucoma surgery. Complications are unusual, but can include:
An infection, bleeding, undesirable changes in intraocular pressure, loss of vision and cataract development
Sometimes, a single surgical procedure is not effective in halting the progress of an person's glaucoma. In these cases, repeat surgery, and/or continued treatment with topical or oral medications may be necessary.